Laparoscopic Surgery
Hernioplasty/Hernia Repair With Mesh (Inguinal/Ventral)
Hernia
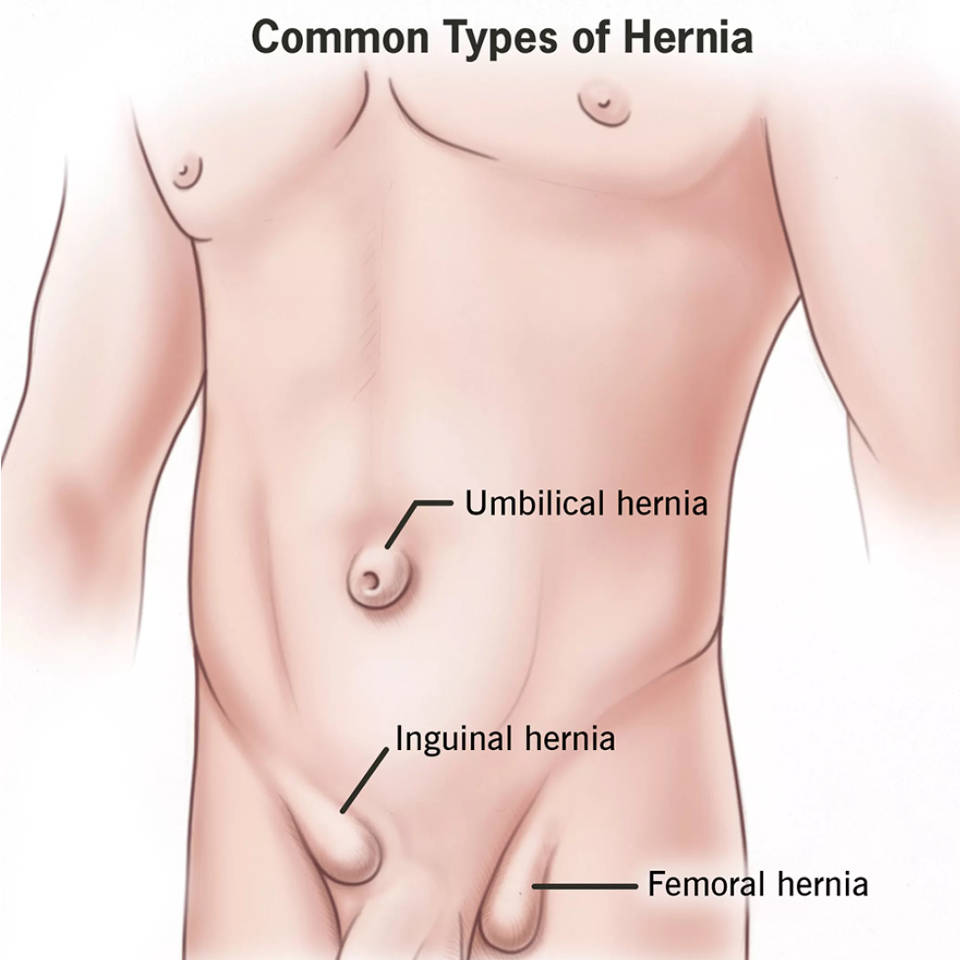
A hernia is an abnormal protrusion(out pouching) of part of body through any weakness in its covering. The image above depicts the most common sites of hernia. A hernia in you groin area is usually an inguinal hernia or less commonly a femoral hernia depending on the exact location.
Any hernia over midline of abdomen is called ventral hernia and if it is at the exact location of umbilicus it is called umbilical hernia. Sometimes if you have had a surgery and there is a hernia at the site of surgery it is known as incisional hernia. There are some rare types of hernia which your clinician would be able to diagnose on examination or by some radiological evaluation like ultrasound or CT scan.
How will I know that I have hernia?
Symptoms caused by hernia are variable.
Most commonly in early stages you might feel discomfort, a feeling of stretch, some dragging sensation or heavyness at the site of hernia. Over a period of time as the hernia increases in size it gradually becomes visible or it comes out whenever you strain at something like sneezing, coughing, straining at stool, lifting heavy weight, bending forward or any such activity which puts pressure on the abdomen. Usually at this initial stage the hernia goes back or it reduces once you rest or lie down.
Gradually it further increases in size and may get visible just on standing and it might get stuck and stop going back. Sometimes at this stage it might become severely painful as it gets swollen and you might be forced to visit emergency because of it. Ideally one should not wait till this stage and should consult a clinician a very onset of the problem.
You may have indigestion, bloating, vomiting, diarrhoea or constipation and you may not feel like eating anything.
If you have any of these symptoms you should consult a doctor who would usually advice an ultrasound examination of the involved area.
Sometimes for further evaluation a CT scan is done.
I had pain which was diagnosed as hernia but it resolved with time on its own. Now I don’t have any pain. What should I do?
It is true that many times pain of hernia resolves with medications and some rest. But one should not ignore if the pain has settled and should opt for surgical intervention as soon as possible. Reason for this is that there is always a chance of recurrence and next time one might end up in complications.
What are the possible complications of hernia?
Hernia might gradually enlarge and at times might increase in size so much that it might affect day to day movement and activity.
If it stops going back it is called irreducible hernia and it might get painful at this stage. If neglected gradually the blood supply to the herniated part becomes hampered and engorgement increases and so does the pain. If intestine has gone through the hernia and it gets blocked then you might develop a condition known as intestinal obstruction and if neglected further it may lead to gangrene of the herniated content and ultimately the intestine might rupture which is a more severe condition where infection spreads to the entire abdomen and will need a bigger incision and bigger surgery known as laparotomy for treatment.
What are the treatment options for hernia?
Universally the treatment for hernia is some form of surgical intervention. As it is a mechanical defect it needs to be closed and to be given some form of reinforcement to prevent recurrence. The reinforcement is in the form of a “MESH” which is placed over the defect and covers some area beyond the defect as well and fixed with some form of stitches or tacks.
Are there different qualities of mesh?
Depending upon the type of hernia there are different variety of mesh and depending upon the brand used the quality might be different.
Usually for inguinal hernia a mesh made of polypropylene is used of varied sizes. In ventral hernia a composite or a dual mesh is needed which is meant to have one side of such a material which does not harm the intestine.
How is the surgery performed for hernia?
The surgical treatment of hernia is by laparoscopic method also known as minimal access/keyhole surgery where the entire process is done through three small punctures in the body. Two punctures are 5mm in size and one is 10mm.
There are various types of procedures which you might discuss with your clinician. In some situations the surgery may be done by conventional open method where an incision is made at the site of hernia for the procedure.
What are the preparations required before surgery and what should I expect during hospital stay and after discharge?
There are two scenarios either you will be operated in emergency or as elective surgery.
If it is elective then the preparation for surgery will be started from the outpatient department (OPD). You will be advised to undergo a few tests to assess your body functions and a pre-anaesthetic check-up (PAC) will be done by an anaesthesiologist (a specialist doctor) who will assess your fitness for anaesthesia.
Most likely you will be admitted on the day of surgery unless you have some specific concerns which warrant some extra stay before the surgery.
You will be advised not to eat or drink anything from midnight of the day prior to surgery and not to eat or drink anything on the morning of admission as well. If you take some medications regularly in the morning than please do not forget to discuss regarding them with your doctor so that he advices you on which medicine to take and which not to take.
Upon admission some paper work will be done and you will be asked to sign consent forms for anaesthesia and surgery.
If it is an emergency situation than all the above process will happen while you are admitted and from here on the further actions are same.
You will be asked to change in to hospital clothing, shaving of the abdomen will be done and you will be given some intravenous medications.
Once the preparations are done you will be wheeled into the preoperative area where nursing staff and doctors will confirm your identity and then you will be shifted to the operating room. Your anaesthetist will put you under general anaesthesia and then surgery will start. Usually it takes about one hour for the surgery to be over and then you will be shifted to post-operative recovery area in conscious state. You will be kept there for couple of hours and then you will be shifted to your designated room.
A catheter (pipe) might be put to drain out urine for maximum 24 hours and will be removed before you are Sent home.
Usually, with few exceptions, once around six hours are over after surgery and you feel comfortable you will be allowed some liquids and later some soft diet will be given.
You will be discharged to home the day after the surgery. You will be advised some medications on your discharge. You will be advised to take soft diet at home for two days and then gradually you can start having normal diet.
Usually if all goes well you will be called for a visit to OPD two days after discharge where the dressing over the stitches will be changed and then five days after discharge you will be called for removal of stitches.
How soon can I resume work after surgery? How much bed rest is advised? Is there any specific season of year when I should opt for surgery?
No bed rest is advised. You will be encouraged to walk about on your own from the next day of surgery. You can resume normal household work two days after surgery. Climbing stairs will not be a problem.
Some activities which are to be avoided completely are forward bending, lifting heavy weight, straining at stools or urine.
You may start driving one week after the surgery.
After a week you can resume walking. For a month you would be advised not to do weight training, running, jogging, cycling, yoga. You can resume all of this gradually after a month from the date of surgery.
Considering that almost all hospitals and households have air conditioning the season has become irrelevant so you can plan surgery as per the need and convenience anytime round the year.