- +91 80764-55085
- info@drgauravshrivastav.com
- Ghaziabad, Uttar-Pradesh 201012 & Rohini, Delhi-110089
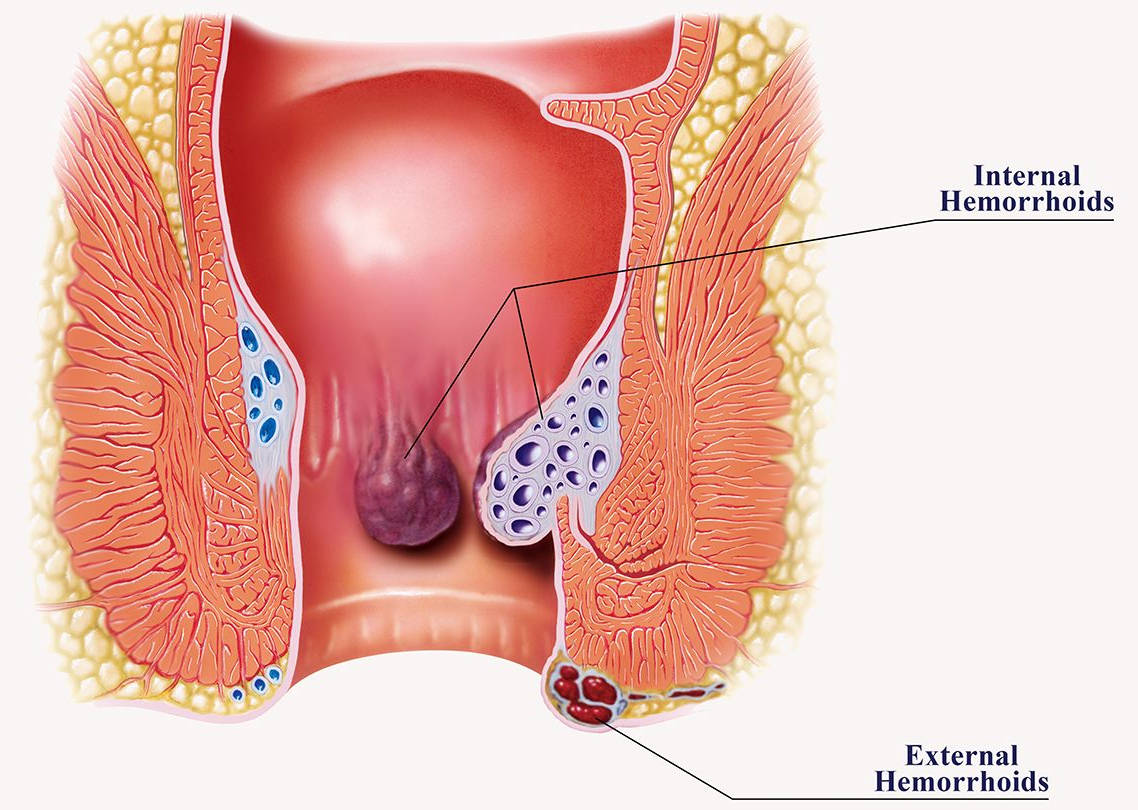
What is Haemorrhoid/Piles?
Haemorrhoids or piles are swollen/engorged veins in lower part of rectum/anal canal.
How will I know that I have haemorrhoids?
One of the most common concern for a visit to a surgeon is a bleeding pile. Patient either presents with bleeding which happens usually after passing motion and is described by the patient as a jet of blood, patient might notice blood while cleaning or in the pan. Many a times bleeding is not visible but over a period of time people develop anaemia.
Second most common presentation of a haemorrhoid is a mass protruding from the anus.
Depending on the stage the mass might come out while passing motion and it reduces back on its own, or it might come out and one is able to push it back or at times it stays out all the time.
If you have any of these symptoms you should consult a doctor who would do a local examination and might do a proctoscopic examination if you feel comfortable.

What are the treatment options for haemorrhoid?
Any treatment dealing with haemorrhoids should be targeted at dealing with the base of haemorrhoids and the hemorrhoidal pedicle where lies the feeding arterial supply of the haemorrhoid. Standard treatment involved tying the pedicle and excising the hemorrhoidal mass which led to formation of large wounds which took a long time to heal and were extremely troublesome for the patient.
Treatment evolved to stapler haemorrhoidectomy where a special single use device is used to deal with the base of haemorrhoid and staple the haemorrhoidal feeding vessels circumferentially. This is a good treatment option considering that there is no external wound, recovery is expedited and patient returns to work early with no frequent visits to the clinic. The only con being that it leaves behind a foreign body in term of staples and rarely might lead to infection, pain, or tenesmus later on. Improper technique might lead to a lower staple line which can be very painful. The only Achilles heel to this is recurrence. If patient is not very compliant or if the procedure is done early in life and later on there is recurrence the clinician is stuck with lack of alternate options.
DIODE laser effectively circumvents all these issues. It is effective in every grade of haemorrhoid. This treatment also does not leave behind any external wound and there is no frequent visit to the clinic. In addition it does not leave behind any foreign body hence negating the chance of complication associated with stapler and in the case of a recurrence the procedure can be easily repeated.
Traditional Haemorrhoidectomy

DIODE laser treatment for Haemorrhoids
